Oral Board Study Guide
*Flash Cards
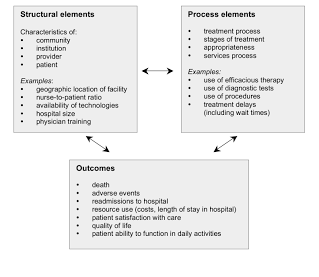
The Donabedian Model
Who: Created by Avedis Donabedian (physician and health services researcher at University of Michigan)
What: A Conceptual Model provides a framework for examining health services quality. The quality of care can be drawn from three categories: “structure,” “process,” and “outcomes." Structure describes the context in which care is delivered, including hospital buildings, staff, financing, and equipment. Process denotes the transactions between patients and providers throughout the delivery of healthcare. Finally, outcomes refers to the effects of healthcare on the health status of patients and populations.
A conceptual model is a model made of the composition of concepts, which are used to help people know, understand, or simulate a subject the model represents.
When: The original model was developed in 1966
What: A Conceptual Model provides a framework for examining health services quality. The quality of care can be drawn from three categories: “structure,” “process,” and “outcomes." Structure describes the context in which care is delivered, including hospital buildings, staff, financing, and equipment. Process denotes the transactions between patients and providers throughout the delivery of healthcare. Finally, outcomes refers to the effects of healthcare on the health status of patients and populations.
A conceptual model is a model made of the composition of concepts, which are used to help people know, understand, or simulate a subject the model represents.
When: The original model was developed in 1966
Andersen Healthcare Utilization Model
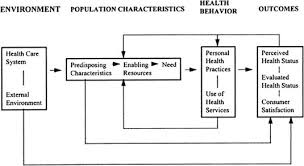
Who: Created by Ronald M. Andersen, a health services professor at UCLA
What: A Conceptual Model provides a framework demonstrating the factors that lead to the use of health services. According to the model, usage of health services (including inpatient care, physician visits, dental care etc.) is determined by three dynamics: predisposing factors, enabling factors, and need. Predisposing factors can be characteristics such as race, age, and health beliefs. For instance, an individual who believes health services are an effective treatment for an ailment is more likely to seek care. Examples of enabling factors could be family support, access to health insurance, one's community etc. Need represents both perceived and actual need for health care services.
A conceptual model is a model made of the composition of concepts, which are used to help people know, understand, or simulate a subject the model represents.
When: The original model was developed in 1968. The original model was expanded through numerous iterations and its most recent form models past the use of services to end at health outcomes and includes feedback loops
What: A Conceptual Model provides a framework demonstrating the factors that lead to the use of health services. According to the model, usage of health services (including inpatient care, physician visits, dental care etc.) is determined by three dynamics: predisposing factors, enabling factors, and need. Predisposing factors can be characteristics such as race, age, and health beliefs. For instance, an individual who believes health services are an effective treatment for an ailment is more likely to seek care. Examples of enabling factors could be family support, access to health insurance, one's community etc. Need represents both perceived and actual need for health care services.
A conceptual model is a model made of the composition of concepts, which are used to help people know, understand, or simulate a subject the model represents.
When: The original model was developed in 1968. The original model was expanded through numerous iterations and its most recent form models past the use of services to end at health outcomes and includes feedback loops
Porter's Five Forces (Managerial Economics)

Who: Created by Michael E. Porter of Harvard University
What: A Conceptual Model provides a framework to analyze level of competition within an industry and business strategy development. It draws upon industrial organization (IO) economics to derive five forces that determine the competitive intensity and therefore attractiveness of an Industry. Attractiveness in this context refers to the overall industry profitability. An "unattractive" industry is one in which the combination of these five forces acts to drive down overall profitability. A very unattractive industry would be one approaching "pure competition", in which available profits for all firms are driven to normal profit.
When: 1979
Where: In 1979, Harvard Business Review published “How Competitive Forces Shape Strategy”
What: A Conceptual Model provides a framework to analyze level of competition within an industry and business strategy development. It draws upon industrial organization (IO) economics to derive five forces that determine the competitive intensity and therefore attractiveness of an Industry. Attractiveness in this context refers to the overall industry profitability. An "unattractive" industry is one in which the combination of these five forces acts to drive down overall profitability. A very unattractive industry would be one approaching "pure competition", in which available profits for all firms are driven to normal profit.
When: 1979
Where: In 1979, Harvard Business Review published “How Competitive Forces Shape Strategy”
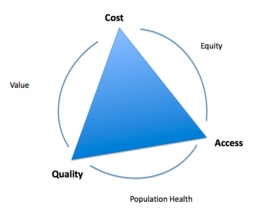
Kissick's Iron Triangle (US Healthcare Systems)
Who: Created by William Kissick MD, a professor of medicine from University of Pennsylvania, who worked on the original Medicare proposal
What: A Conceptual Model provides a framework demonstrating the relationship between cost, quality, and access in all sorts of institutions such as policy making, healthcare, and businesses. You can't affect one aspect without affecting the other two aspects, it is a concept full of trade-offs. Being that the relationship is reciprocal it is difficult to have any significant change in either cost, quality, or access.The problem with this is that they are in competition with each other. The iron triangle later became the intellectual forerunner of today’s Triple Aim framework For example, to make healthcare more affordable would increase access to it but most likely decrease the quality of care. You might increase the quality of the healthcare, but that will increase costs and limit access to it. You could also increase access to the healthcare, but that will cost money, or result in lower quality care..
"Health policy analysts commonly refer to an “iron triangle” of health care. The three vertices of the triangle are the cost, quality, and accessibility of care. The “iron triangle” means that, in equilibrium, increasing the performance of the health care system along any one of these dimensions can compromise one or both of the other dimensions, regardless of the amount that is spent on health care. Such tradeoffs are not always required, of course. For example, tying payments to health care providers to the quality of services provided could improve providers’ incentives to contain costs and improve quality. Better quality also could be achieved at less cost by reducing unnecessary services and managing consumers with chronic conditions more cost-effectively. Competition has an important role to play in accomplishing these objectives."
(From WILLIAM L. KISSICK, MEDICINE’S DILEMMAS: INFINITE NEEDS VERSUS FINITE RESOURCES 1994).
When: First introduced in William Kissick’s novel, Medicine’s Dilemmas: Infinite Needs Versus Finite Resources
Where: 1994
Weaknesses: Author and family physician David Liu, M.D. wrote of the Iron Triangle as not a law binding the healthcare system but an observation that the healthcare system is currently stuck in and can be broken. He compares healthcare to notable inventions in history, such as commercial flight and computers. When both first existed they were unaffordable to the public which restricted access and were not of the best or safest quality. They each went through their own "Iron Triangle" phases where cost, quality, and access fluctuated but ultimately here we are with the most most affordable, widely accessible, and powerful forms of computing and transportation in the history of mankind. Dr. Liu's theory is that healthcare hasn't reached it's peak and we just need future doctors, insurers, entrepreneurs, and patients to discover what these changes need to be made to achieve the maximum balance between the three.
Critics of the Iron Triangle state that the model is not actually as rigid as its name indicates, but is more dynamic because costs of care are constantly changing. Health care costs change faster than the other two dimensions of the triangle, affecting access to care, which in turn influences quality. Other skeptics argue that the Iron Triangle is not a fixed framework, but an observation and reflection of the current state of health care. In line with Clayton Christensen’s theory on disruptive innovation, critics of the Iron Triangle believe that health care, particularly in the United States, has not yet been disrupted like fields such as computer production. The belief is that with time and innovation, the current Iron Triangle will be disrupted, and just as the cost of computer production has fallen as quality and access to computers has increased, health care access and quality will rise, and cost will decrease. Critics argue that the Iron Triangle is not a one-size-fits-all model that can be applied to an entire population.
What: A Conceptual Model provides a framework demonstrating the relationship between cost, quality, and access in all sorts of institutions such as policy making, healthcare, and businesses. You can't affect one aspect without affecting the other two aspects, it is a concept full of trade-offs. Being that the relationship is reciprocal it is difficult to have any significant change in either cost, quality, or access.The problem with this is that they are in competition with each other. The iron triangle later became the intellectual forerunner of today’s Triple Aim framework For example, to make healthcare more affordable would increase access to it but most likely decrease the quality of care. You might increase the quality of the healthcare, but that will increase costs and limit access to it. You could also increase access to the healthcare, but that will cost money, or result in lower quality care..
"Health policy analysts commonly refer to an “iron triangle” of health care. The three vertices of the triangle are the cost, quality, and accessibility of care. The “iron triangle” means that, in equilibrium, increasing the performance of the health care system along any one of these dimensions can compromise one or both of the other dimensions, regardless of the amount that is spent on health care. Such tradeoffs are not always required, of course. For example, tying payments to health care providers to the quality of services provided could improve providers’ incentives to contain costs and improve quality. Better quality also could be achieved at less cost by reducing unnecessary services and managing consumers with chronic conditions more cost-effectively. Competition has an important role to play in accomplishing these objectives."
(From WILLIAM L. KISSICK, MEDICINE’S DILEMMAS: INFINITE NEEDS VERSUS FINITE RESOURCES 1994).
When: First introduced in William Kissick’s novel, Medicine’s Dilemmas: Infinite Needs Versus Finite Resources
Where: 1994
Weaknesses: Author and family physician David Liu, M.D. wrote of the Iron Triangle as not a law binding the healthcare system but an observation that the healthcare system is currently stuck in and can be broken. He compares healthcare to notable inventions in history, such as commercial flight and computers. When both first existed they were unaffordable to the public which restricted access and were not of the best or safest quality. They each went through their own "Iron Triangle" phases where cost, quality, and access fluctuated but ultimately here we are with the most most affordable, widely accessible, and powerful forms of computing and transportation in the history of mankind. Dr. Liu's theory is that healthcare hasn't reached it's peak and we just need future doctors, insurers, entrepreneurs, and patients to discover what these changes need to be made to achieve the maximum balance between the three.
Critics of the Iron Triangle state that the model is not actually as rigid as its name indicates, but is more dynamic because costs of care are constantly changing. Health care costs change faster than the other two dimensions of the triangle, affecting access to care, which in turn influences quality. Other skeptics argue that the Iron Triangle is not a fixed framework, but an observation and reflection of the current state of health care. In line with Clayton Christensen’s theory on disruptive innovation, critics of the Iron Triangle believe that health care, particularly in the United States, has not yet been disrupted like fields such as computer production. The belief is that with time and innovation, the current Iron Triangle will be disrupted, and just as the cost of computer production has fallen as quality and access to computers has increased, health care access and quality will rise, and cost will decrease. Critics argue that the Iron Triangle is not a one-size-fits-all model that can be applied to an entire population.
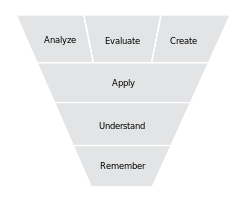
Bloom's Taxonomy Model
Who: It is named after Benjamin Bloom, who chaired the committee of educators that devised the taxonomy. He also edited the first volume of the standard text, Taxonomy of Educational Objectives: The Classification of Educational Goals.[1]
What: A way of distinguishing the fundamental questions within the education system.
refers to a classification of the different objectives that educators set for students (learning objectives). It divides educational objectives into three "domains": cognitive, affective, and psychomotor (sometimes loosely described as "knowing/head", "feeling/heart" and "doing/hands" respectively). Within the domains, learning at the higher levels is dependent on having attained prerequisite knowledge and skills at lower levels. A goal of Bloom's taxonomy is to motivate educators to focus on all three domains, creating a more holistic form of education.
When and Where: The first volume of the taxonomy, "Handbook I: Cognitive" (Bloom et al. 1956) was published in 1956. "Handbook II: Affective" (Krathwohl, Bloom & Masia 1965) followed in 1965. A third volume, for the psychomotor domain, was planned, but never published. Other educators created their own taxonomies within this domain, including Simpson (1966), Harrow (1972) and Dave (1975). A revised version of the taxonomy for the cognitive domain was created in 2000.
What: A way of distinguishing the fundamental questions within the education system.
refers to a classification of the different objectives that educators set for students (learning objectives). It divides educational objectives into three "domains": cognitive, affective, and psychomotor (sometimes loosely described as "knowing/head", "feeling/heart" and "doing/hands" respectively). Within the domains, learning at the higher levels is dependent on having attained prerequisite knowledge and skills at lower levels. A goal of Bloom's taxonomy is to motivate educators to focus on all three domains, creating a more holistic form of education.
When and Where: The first volume of the taxonomy, "Handbook I: Cognitive" (Bloom et al. 1956) was published in 1956. "Handbook II: Affective" (Krathwohl, Bloom & Masia 1965) followed in 1965. A third volume, for the psychomotor domain, was planned, but never published. Other educators created their own taxonomies within this domain, including Simpson (1966), Harrow (1972) and Dave (1975). A revised version of the taxonomy for the cognitive domain was created in 2000.
IHI Triple Aim
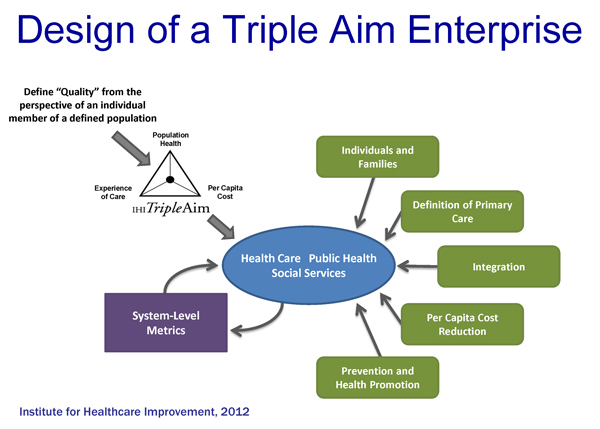
Who: Developed by the Institute for Healthcare Improvement in Cambridge, Massachusetts
What:
The IHI Triple Aim is a framework that describes an approach to optimizing health system performance. It is IHI’s belief that new designs must be developed to simultaneously pursue three dimensions, which we call the “Triple Aim”:
In 2008 Don Berwick, Tom Nolan, and John Whittington first described the Triple Aim of simultaneously improving population health, improving the patient experience of care, and reducing per capita cost. The Institute for Healthcare Improvement (IHI) developed the Triple Aim as a statement of purpose for fundamentally new health systems that contribute to the overall health of populations while reducing costs.
When: Created in 2007
Where: Cambridge, Massachusetts
Good stuff to compare triple aim and iron triangle right here
What:
The IHI Triple Aim is a framework that describes an approach to optimizing health system performance. It is IHI’s belief that new designs must be developed to simultaneously pursue three dimensions, which we call the “Triple Aim”:
- Improving the patient experience of care (including quality and satisfaction);
- Improving the health of populations; and
- Reducing the per capita cost of health care
In 2008 Don Berwick, Tom Nolan, and John Whittington first described the Triple Aim of simultaneously improving population health, improving the patient experience of care, and reducing per capita cost. The Institute for Healthcare Improvement (IHI) developed the Triple Aim as a statement of purpose for fundamentally new health systems that contribute to the overall health of populations while reducing costs.
When: Created in 2007
Where: Cambridge, Massachusetts
Good stuff to compare triple aim and iron triangle right here
